
Holcomb C3-R Versus Other Corneal Cross-Linking Procedures for Keratoconus
What is Corneal Collagen Cross-linking?
Keratoconus is a weakening of the collagen in the cornea, causing the cornea to steepen, which decreases vision. Corneal Cross-linking is a specialized treatment that strengthens the collagen and corneal structure, and if done properly with the proper technique, it can halt the progression of vision loss for many years.
Most Important Considerations for Corneal Collagen Cross-linking
- Does the procedure halt the progression of vision loss, that is, what is the stability of the procedure for both short term and long term success?
- What is the level of Keratoconus vision loss at treatment time?
- Is the procedure invasive, that is, does any layer of the cornea need to be removed for the procedure?
- What is the complication rate?
- How long does it take?
- Can both eyes be treated at the same time?
- Is it covered by insurance?
- What is the recovery time?
- Is there published data showing both short-term (1-year or less) and long-term (1 year to 5 years) halting of the vision loss progression?
- Can both eyes be treated at once?
- Can I wear my contacts immediately after the treatment?
Long Term Stability
Long term stability is the most important factor for evaluating the success for any type of cross-linking procedure. Since the goal of cross-linking is to stabilize Keratoconus from further progression, the question to ask is “What is the long-term stability rate?” Since Keratoconus is a progressive disease that causes the cornea to steepen, it’s important to know the percentage of patients whose corneas were stabilized, ie, arresting the steepening over time should be the primary outcome. (See Ng, Ren, Lindsley, Hawkins, & Kuo. Cochrane Database Syst Rev 2021). Reporting one-year stability results is not sufficient to characterize the long term success of stabilizing Keratoconus. If 100 patients had a type of cross-linking that had only one-year data on stability, it’s likely that many more patients will move from stabilized Keratoconus to progressive Keratoconus over the next 5 or 10 years because that is the nature of Keratoconus, when lower UV energy levels are used for cross-linking.
As mentioned above, stability is perhaps the most important variable for deciding which procedure to have for Keratoconus treatment.
Data shows Holcomb C3-R had 99.3% stability short term and long term (See Chan & Boxer Wachler. Therapeutic Options for Keratoconus and Corneal Ectasia 2007 and Vicente & Boxer Wachler. American Society of Cataract and Refractive Surgery Annual Meeting, April 2010), CXL had only 73.1% stability short term (See NDA 203-324, FDA Advisory Committee Briefing Package, February 24, 2015) and data shows 14% retreatments occurred for long term (See Raiskup, Herber, Lenk, Ramm Amer J Ophthalmol 2023) and no studies applying Epioxa provide data on stability. (See FDA Epioxa Highlights of Prescribing Information 2025).
Holcomb C3-R
Holcomb C3-R is a non-invasive cross-linking procedure that uses adjustable UV light to titrate the degree of corneal cross-linking in the cornea. The procedure is named after Olympic athlete Steven Holcomb following his historic Olympic gold medal win for the United States as the bobsled driver after his Keratoconus was treated, thereby ending a 62-year Olympic gold medal drought for the U.S. Holcomb C3-R is a 30-minute procedure that was developed in 2003, making it the first non-invasive “epi-on” cross-linking procedure. Performing cross-linking with this approach has many advantages including:
- Both eyes can be treated at the same time. Because Holcomb C3-R is non-invasive, the recovery for patients is usually only one day. This allows both eyes to be treated simultaneously since both eyes should be fully recovered by the next morning.
- The procedure is painless.
- Special agents added to the riboflavin solution have been shown to enable riboflavin to penetrate intact epithelium without the need to remove the epithelium (See Zhang, Sukthankar, Tomich & Conrad. Invest Ophthalmol Vis Sci 2012).
- No complications have been reported since the development of Holcomb C3-R in 2003.
- Patients can return to wearing contact lenses the next day following the procedure.
- Long term stability rate is very high at 99.3% with a single treatment for stopping the progression of Keratoconus.

Important: Holcomb C3-R was first performed more than 20 years ago in 2003 and published data shows a 99.3% rate of stabilizing Keratoconus progression. Data also indicates that when Holcomb C3-R is performed in conjunction with and on the same day as Intacs, the Intacs flattening and visual improvement effect is enhanced by Holcomb C3-R. (See Chan, Sharma, & Boxer Wachler. J Cataract Refract Surg 2007). A 20-year track record of stability has not been reported for CXL or Epioxa cross-linking procedures.
Invasive Cross-linking: Epi-off vs. Epi-on
CXL Epi-Off Cross-linking
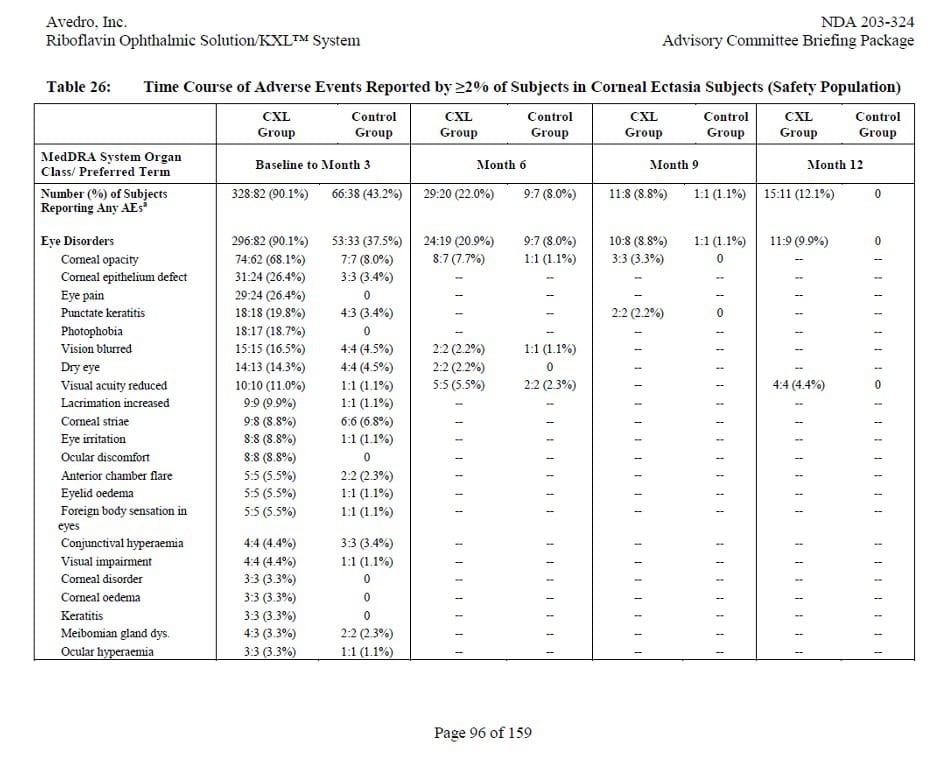
Many ophthalmologists perform CXL cross-linking where the surface cornea epithelium is removed because of the high viscosity level of riboflavin used in that procedure, due to its content of dextran (a thickening agent) that prevents riboflavin from penetrating the corneal collagen through the epithelium. Removing the epithelium is invasive and creates specific risks, and the resultant complications have been reported in the published data (See NDA 203-324, FDA Advisory Committee Briefing Package, February 24, 2015. For the specific data, see the table below).


Holcomb C3-R Vs Epi-Off CXL
The CXL procedure created eye problems, > 90%, within the first 3 months, including cornea infections, scarring, loss of best-corrected vision, cornea nerve damage, eye pain, dry eyes, tearing, inflamed corneas, foreign body sensation, and red eyes. Between 3 months and 6 months after treatment, 20% of patients continued to experience eye problems. Voluminous clinical research shows epi-off CXL carries significant risks of complications. (See NDA 203-324, FDA Advisory Committee Briefing Package, February 24, 2015)
As discussed above, stabilization of the corneal steepening and stoppage of vision loss is the critical factor in evaluating the proper procedure for your eye care treatment. The chart below shows the high level of patients that continue to progress after CXL treatment.

Not Best Use
Epi-off CXL should NOT be used in patients with relatively good best-corrected vision because the risks of adverse side effects can lead to worsening of vision. Patients with very thin corneas should not undergo epi-off CXL because of potential damage to the cornea endothelium as it is removed for treatment.
Other Considerations
Cost: Most insurances now consider cross-linking medically necessary. Some practices are not set up to directly bill insurance companies and those offices can provide superbills to patients to submit to their insurance company for consideration of reimbursement.
Rule of Thumb
As a rule of thumb, if cross-linking where no epithelium is removed is not available, then other types of cross-linking, such as CXL, may be useful to attempt to stabilize the vision loss associated with Keratoconus and warrant the risks of the procedure.
Non-Invasive Cross-linking: Holcomb C3-R vs Epioxa
There are other cross-linking procedures that do not require the removal of the epithelium. One example is Epioxa, where complications are reduced, but not eliminated. Even though the epithelium is not removed, it is manipulated and softened to aid in the absorption of the riboflavin. This disruption during Epioxa can still be painful and requires a contact lens to be used after treatment to help the epithelium heal. Further, disrupting the epithelium can increase risks of the procedure. Additionally, only one eye can be treated at a time. Adverse side effects with Epioxa occur in 5 to 25% of patients which ranged from corneal opacity (haze), photophobia, punctate keratitis, eye pain, eye irritation, lacrimation increased, corneal epithelium defect, eyelid swelling, corneal striae, visual acuity reduction, dry eye, and anterior chamber flare. (See EPIOXA HIGHLIGHTS OF PRESCRIBING INFORMATION 10/25).
Most importantly, limited to no data is available concerning the long term viability of the treatment to stabilize vision loss. A number of prominent scholars have suggested that the treatment time, even though at a more intense level, does not provide adequate outcome for Keratoconus stabilization (See Kandel, Abbondanza, Gupta et al. Eye (London) 2023).
Not Best Use
For patients who would like the epithelium to remain intact during the procedure, Epoixa is not the best choice.
Other Considerations
Cost: Most insurances do not cover Epioxa. Many practices cannot directly bill insurance companies for the procedure and they provide a bill to patients who then must submit to their insurance company for consideration of reimbursement.
Rule of Thumb
Check with your eye surgeon about the insurance coverage and epithelium involvement before making a decision about the procedure.
Holcomb C3-R
Not Best Use
Holcomb C3-R should not be used in patients who are unable to remain cooperative during the 30-minute procedure. NOTE: Special needs patients may require oral sedatives like Valium to enable cooperation.
Rule of Thumb
As a rule of thumb, if patients with mild, moderate, and advanced stage Keratoconus desire cross-linking where the epithelium is not removed or disrupted during the procedure, and with the longest track record of stabilization since 2003, then Holcomb C3-R is indicated.
Other Considerations
Cost: Most insurances cover Holcomb C3-R.
| Holcomb C3-R | CXL | Epioxa | |
| Considerations | The recovery is 1-day due to the entirely non-invasive nature of Holcomb C3-R. This enables both eyes to be treated at the same time. For patients who wear contact lenses, they can resume wearing contact lenses the next day in both eyes. | Epi-off CXL requires planning for long recovery as the epithelium can require weeks to months to fully heal and stabilize. For this reason, only one eye should be treated at a time until the first eye has completely recovered. | Epioxa requires planning for one eye treated at a time and placement of a contact lens to aid the epithelium to heal. Sunglasses may be needed for light sensitivity. Patients should contact their doctor if they experience severe pain or sudden loss of vision in the treated eye. The second eye should be treated after the first eye is completely recovered and functional. |
Holcomb C3-R Best Use: Holcomb C3-R is best for patients at any stage of Keratoconus because the UV light energy level is adjustable, which allows the amount of cross-linking to be customized per patient. Holcomb C3-R is best for combining cross-linking on the same day with Intacs, CAIRS, and CTAK cornea implants.
CXL Best Use: Epi-off CXL should be used when there is no access to epi-on cross-linking.
Epioxa Best Use: Epioxa should be considered when there is no access to other types of cross-linking.